What Healthcare Providers Need to Know
The Centers for Medicare & Medicaid Services (CMS) has released the proposed 2026 Medicare Physician Fee Schedule (PFS) rule, outlining a 2.5% increase in Medicare physician payment rates for the upcoming year. This important update includes significant reforms such as the introduction of the mandatory Ambulatory Specialty Model (ASM), aimed at specialists treating chronic conditions like low back pain (LBP) and congestive heart failure (CHF). Along with these changes, CMS advances behavioral health billing codes, updates the Medicare Shared Savings Program (MSSP), and refines the Quality Payment Program (QPP) including Merit-Based Incentive Payment System (MIPS) requirements. This blog provides a thorough overview of the CMS’s major 2026 Medicare payment updates, helping physicians and healthcare providers prepare for these changes.
2026 Medicare Physician Fee Schedule Payment Increase Overview
CMS proposes a 2.5% increase in the Medicare Physician Fee Schedule (PFS) conversion factor for calendar year 2026, delivering a much-anticipated boost to physician payments. Advanced Alternative Payment Model (APM) participants are slated to receive an even larger 3.8% payment increase, recognizing their involvement in value-based care initiatives. These updates reflect CMS’s commitment to supporting healthcare providers amid rising operational costs while maintaining sustainable Medicare spending growth.
Details on the New Ambulatory Specialty Model (ASM) for Specialists
One of the landmark proposals in the 2026 Medicare Physician Fee Schedule is the rollout of the Ambulatory Specialty Model (ASM), a mandatory, Innovation Center model starting January 1, 2027. Designed for specialists managing chronic conditions such as low back pain and congestive heart failure, ASM holds individual clinicians accountable for quality and cost performance.
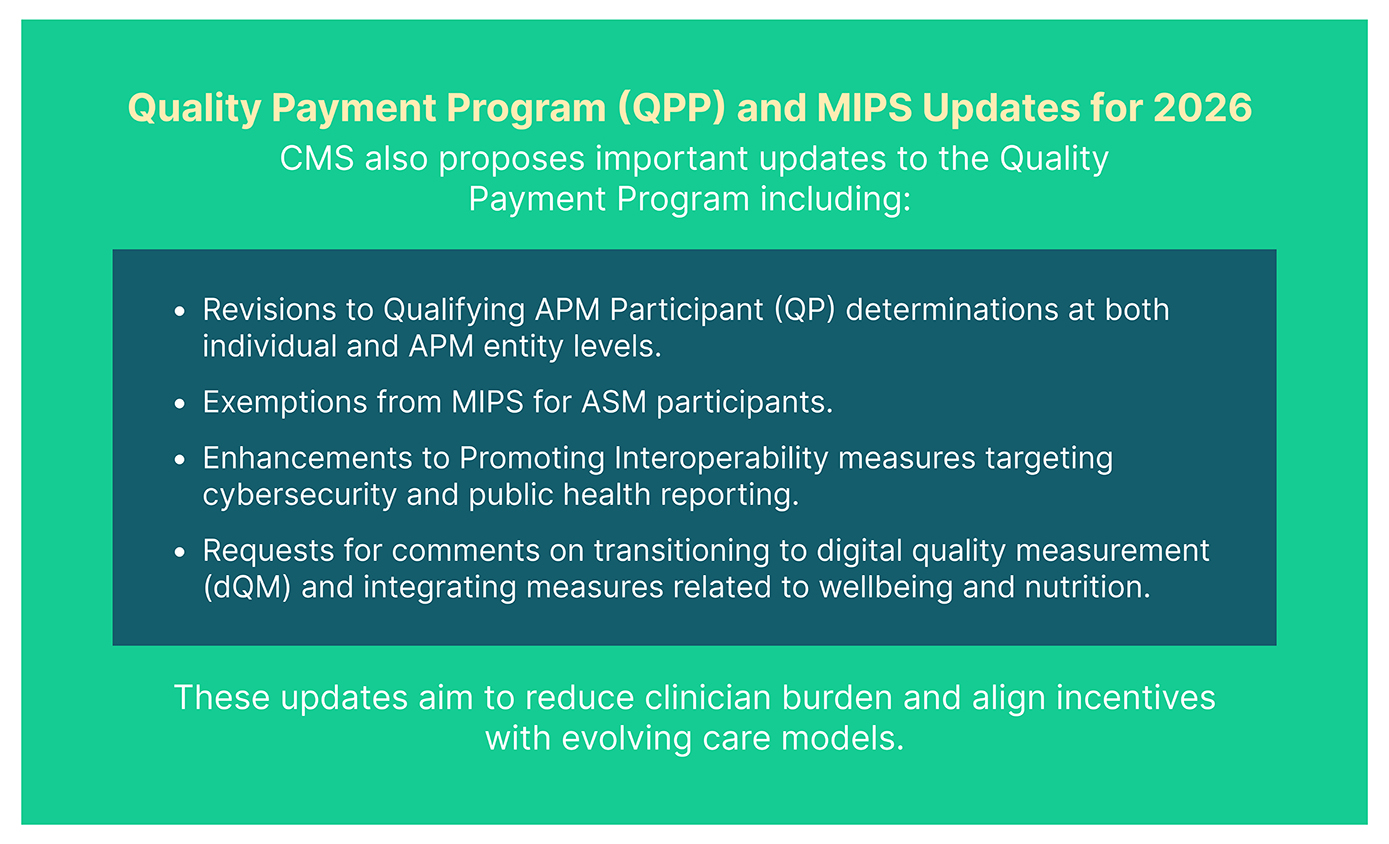
Eligible specialists, including cardiologists, anesthesiologists, orthopedists, and pain management providers, are required to participate if they have treated 20 or more Medicare fee-for-service (FFS) patients with these conditions. This model introduces two-sided financial risk, tying Medicare Part B payments to specialist performance on quality metrics, cost reductions, and care coordination efforts. ASM participants will also benefit from exemption from traditional MIPS reporting requirements during participation years.
Behavioral Health Billing Codes and APCM Updates
Although Advanced Primary Care Management (APCM) is an established Medicare service, CMS proposes new behavioral health add-on billing codes to enhance reimbursement for integrated behavioral health services. These add-ons remove time-based restrictions for billing Collaborative Care Model (CoCM) and behavioral health integration codes alongside APCM, facilitating broader adoption and improved behavioral health integration in primary care.
Telehealth, Digital Health, and AI Payment Policy Expansion
CMS continues to modernize Medicare by expanding payment policies for digital health:
- Broadening coverage for digital mental health devices, including those treating ADHD.
- Simplifying service additions to the Medicare Telehealth Services List.
- Requesting feedback on payment approaches for emerging technologies such as Software as a Service (SaaS) and artificial intelligence (AI) tools in outpatient care.
These initiatives promote innovation and accessibility in Medicare-covered services.
Leveraging Advanced Digital Solutions with Persivia to Navigate 2026 Medicare Physician Fee Schedule Changes
In response to the evolving Medicare Physician Fee Schedule (PFS) for 2026, healthcare providers must adopt sophisticated tools to optimize reimbursement, meet new care coordination mandates, and excel in emerging payment models such as the ASM and APCM.
Persivia’s CareSpace® platform, built on 15 years of expertise, offers advanced AI-powered capabilities that transform complex regulatory challenges into actionable opportunities for payment optimization. With real-time analytics of patient records and automated quality measure tracking, CareSpace® processes vast clinical and financial data streams to help organizations optimize risk adjustment methodologies and capture appropriate reimbursements under the 2026 PFS.
The platform’s robust population health analytics align seamlessly with CMS’s enhanced care coordination requirements, enabling practices to identify high-risk patient cohorts, anticipate care needs, and implement proactive interventions. As CMS shifts the focus from time-based to outcomes-based care management, CareSpace®’s data insights facilitate demonstration of quality improvements pivotal for securing enhanced Medicare payments.
Ready to optimize your Medicare payment strategy? Contact Persivia today to learn how we can help your practice maximize reimbursements under the new 2026 Physician Fee Schedule and excel in value-based care.
Frequently Asked Questions
1. When will the 2026 Medicare physician payment changes take effect?
Most changes, including the 2.5% payment increase, take effect January 1, 2026. However, the Ambulatory Specialty Model begins January 1, 2027, with payment adjustments starting in 2029.
2. Who must participate in the Ambulatory Specialty Model?
Specialists who have treated 20 or more Medicare fee-for-service patients for congestive heart failure (cardiologists) or low back pain (anesthesiologists, pain management, orthopedists, neurosurgeons, PM&R specialists) over a 12-month period in designated geographic areas.
3. How will the payment increases affect my practice?
Qualifying APM participants receive a 3.83% increase, while non-qualifying providers receive a 3.62% increase. The actual impact depends on your specialty mix, with procedure-based specialties potentially seeing slight decreases due to the efficiency adjustment.
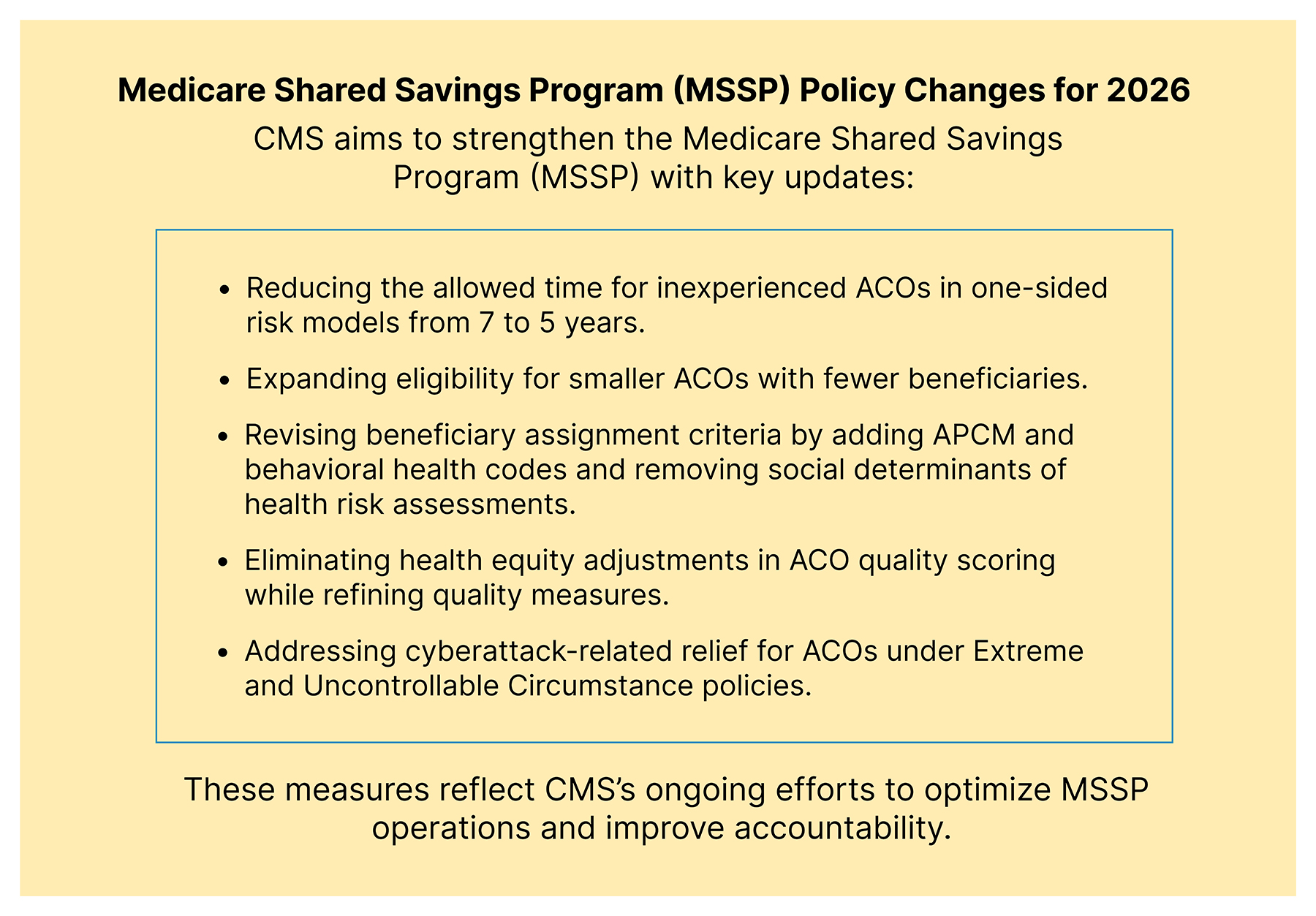
4. Can ACOs with fewer than 5,000 beneficiaries still participate in MSSP?
Yes, starting January 1, 2027, ACOs can participate with fewer than 5,000 beneficiaries in Benchmark Years 1 and 2, but must have at least 5,000 in Benchmark Year 3. These ACOs face reduced shared savings opportunities and capped financial exposure.
5. What happens to the health equity adjustment for ACO quality scores?
The health equity adjustment is eliminated beginning in performance year 2025. CMS believes this change aligns with administration priorities to streamline regulations, though the underlying benchmark adjustment methodology remains unchanged.
6. How does the new skin substitute payment policy work?
Instead of paying individual Average Sales Prices (often over $1,000/cm²), CMS will pay a uniform rate of $125.38 per square centimeter across three FDA-based categories. This applies to incident-to supplies rather than individual product pricing.
7. Will ASM overlap with existing Medicare models like MSSP?
Yes, CMS intentionally designed ASM to overlap with Advanced APMs and other Innovation Center models. However, payment reconciliation methods to prevent double payments remain unclear and require further clarification.
8. What are the new behavioral health integration opportunities?
The three new GPCM add-on codes allow billing behavioral health integration and Collaborative Care Model services alongside Advanced Primary Care Management without time-based requirements, reducing documentation burden and improving access.
Table of Contents