The CJR-X Model would make every IPPS hospital in the country financially accountable for joint replacement episodes from the day of surgery through 90 days post-discharge. Here is what health systems, ACOs, and care teams need to start preparing for.
On April 10, 2026, CMS released its Fiscal Year 2027 IPPS proposed rule, and inside it sits a proposal that will change how hospitals, health systems, and ACOs manage one of Medicare’s most common surgical procedures. The CJR-X (Comprehensive Care for Joint Replacement Expanded) Model would be the first mandatory, nationwide episode-based payment model in Medicare history, covering lower extremity joint replacement (LEJR) surgeries at virtually every IPPS-paid hospital across the country.
For hospital CFOs, CMOs, orthopedic service line leaders, and population health teams, this is not something to track from a distance. If finalized, participation begins October 1, 2027. Preparation needs to start well before that date.

What Is the CJR-X Model, and Who Does It Affect?
CJR-X is the proposed expansion of the original Comprehensive Care for Joint Replacement (CJR) Model, which concluded on December 31, 2024. Where the original program covered hospitals in just 34 Metropolitan Statistical Areas, CJR-X would reach nearly all IPPS hospitals nationwide. The only hospitals excluded at launch are those already enrolled in the mandatory Transforming Episode Accountability Model (TEAM).
The procedural scope grows too. Total hip and knee replacements are now covered in both inpatient and outpatient hospital settings, and ankle replacements enter the bundle for the first time.
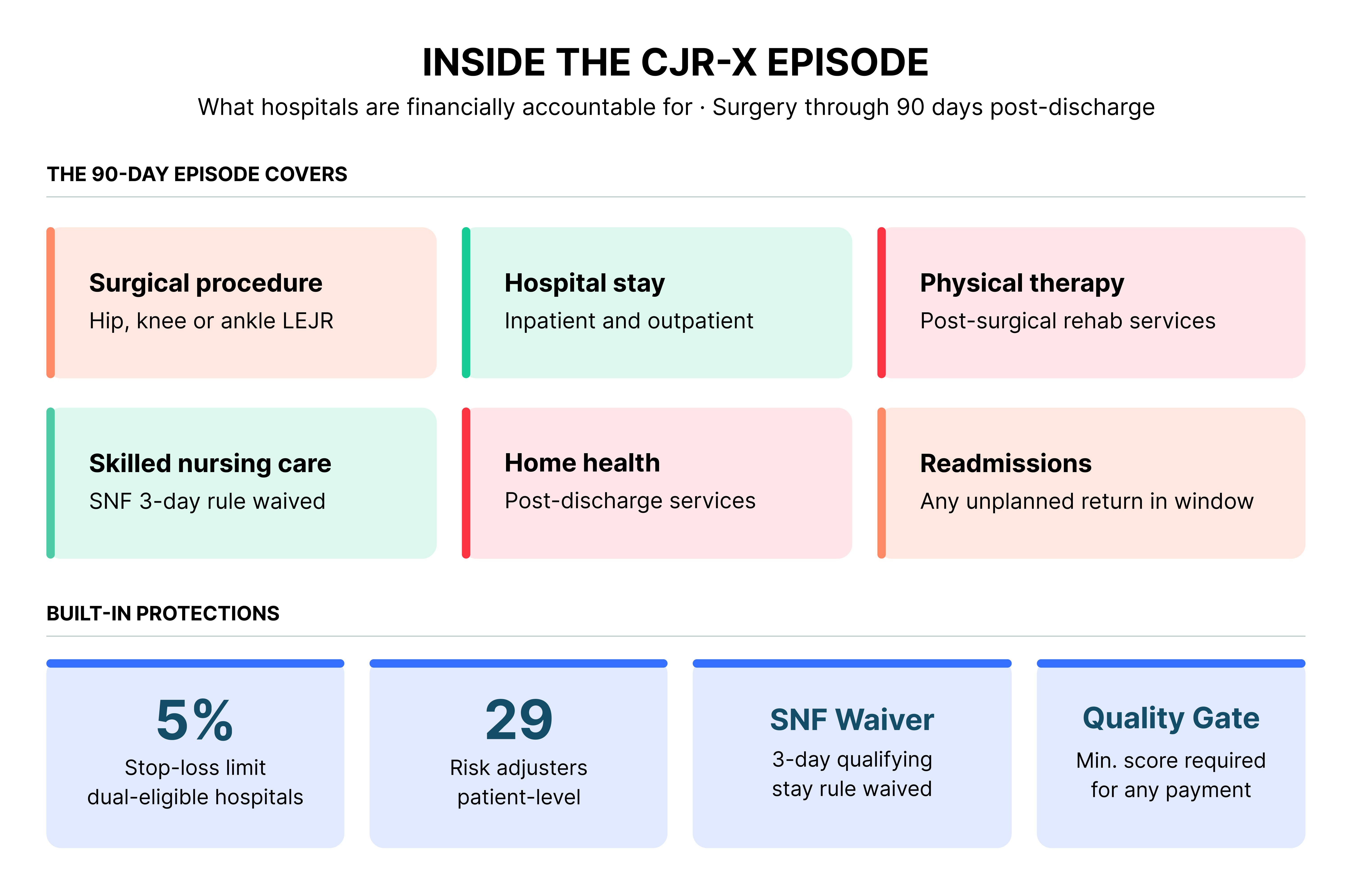
Under the CJR-X model, the participating hospital becomes the single accountable entity for all Medicare Part A and Part B spending tied to the LEJR episode: the procedure, the hospital stay, post-discharge physical therapy, follow-up visits, skilled nursing facility care, home health services, and any readmissions within the 90-day window. All providers continue billing under existing Medicare payment systems. Reconciliation at year-end then determines whether a hospital receives a bonus payment or owes money back to CMS.
How CMS CJR-X Model Reconciliation Works?
At the end of each performance year, CMS compares a hospital’s actual total episode spending against a risk-adjusted target price. If actual spend falls below target and the hospital meets quality thresholds, a shared savings payment is issued. If actual spend exceeds target, the hospital may owe a portion back to Medicare. A 5% stop-loss limit applies to hospitals with large dual-eligible populations. All hospitals must clear a minimum quality score before receiving any reconciliation payment.
A Decade of Evidence Behind the CJR-X Expansion
CMS has strong evidence base for this move. The original CJR program ran from April 2016 through December 2024 and consistently demonstrated that bundled payments can reduce costs without harming patient outcomes. The most recent independent evaluation covered performance years 6 and 7 (2021 through 2023).
“The CJR Model generated an estimated $112.7 million in net Medicare savings while maintaining quality for over 98,000 knee and hip replacement patients across 323 hospitals.”
CMS Innovation Center, April 2026
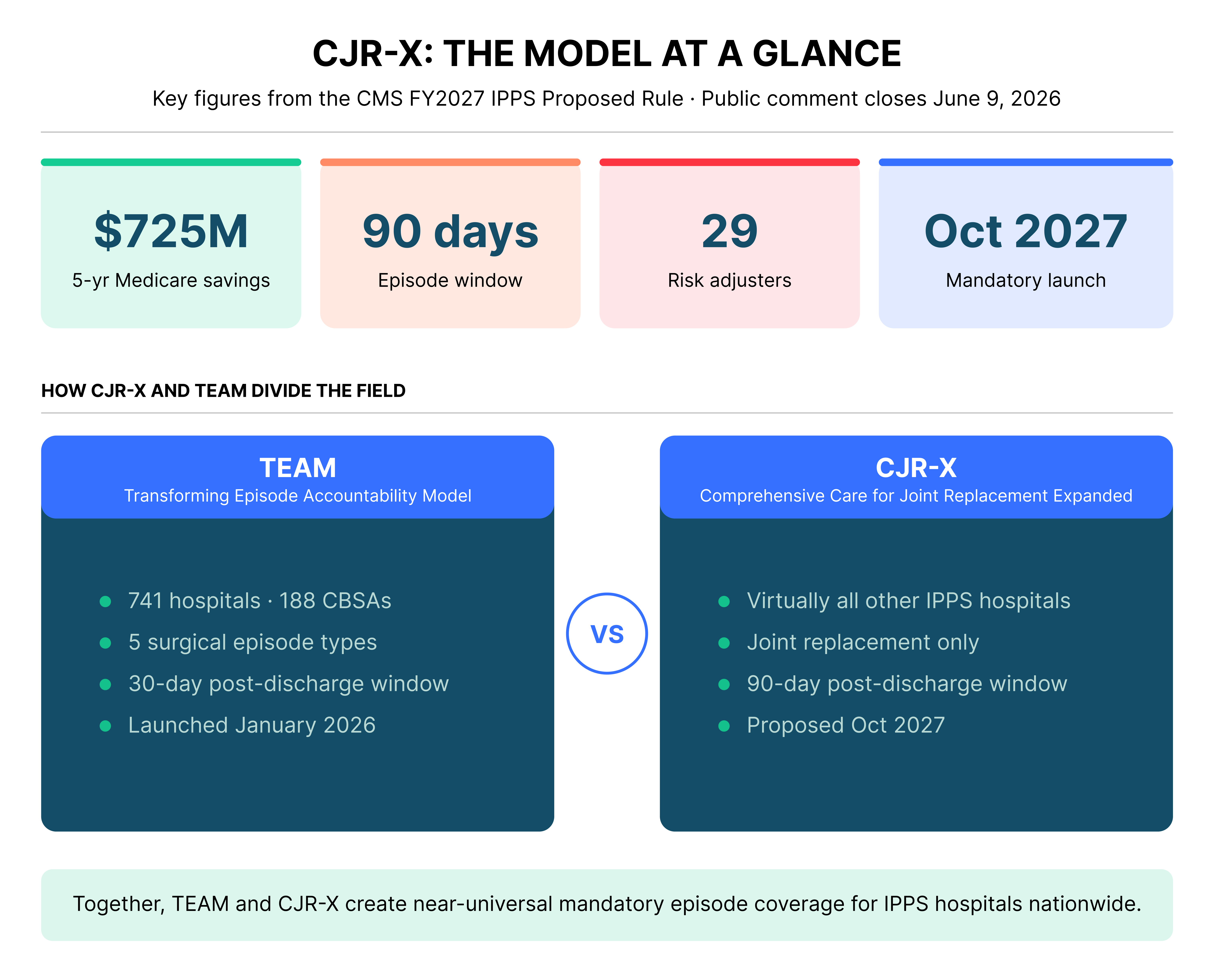
Savings were driven primarily by reductions in post-acute care spending, with a measurable shift away from skilled nursing facilities and toward home health and outpatient rehabilitation settings. There were no adverse effects on complications, mortality, or readmission rates. That track record is the foundation CJR-X is built on. CMS projects the expanded model will generate $725 million in net Medicare savings over its first five performance years.
What CMS is Asking Hospitals to do Under CJR-X
The agency has been direct about the behavioral changes the model is designed to produce. According to CMS, the CJR-X Model would encourage hospitals to work as a team with physicians and post-acute care providers, coordinate care across transitions from the initial procedure through recovery and produce high-value care by reducing unnecessary or duplicative services such as avoidable hospital readmissions.
Structural Safeguards Built into the CMS CJR-X
CMS has built meaningful refinements into CJR-X based on stakeholder feedback from the original program. The risk adjustment methodology now includes 29 adjusters, compared to just 3 in the original CJR, providing far more granular accounting for patient complexity. A 5% stop-loss limit protects hospitals with large dual-eligible populations from outsized downside exposure. Quality-linked payment thresholds ensure that cost reduction cannot come at the expense of clinical outcomes. CJR-X also includes a waiver of the Medicare SNF 3-day qualifying inpatient stay rule, giving hospitals flexibility to place appropriate patients directly into skilled nursing care after an outpatient procedure without triggering a coverage gap.
Hospital associations have pushed back on the mandatory structure. The American Hospital Association has argued that mandatory models present significant challenges, particularly for hospitals that lack the scale or financial capacity to invest in care redesign. The Federation of American Hospitals acknowledged the 2.4% IPPS rate increase as a step forward but noted it falls short of offsetting inflation and rising uncompensated care costs.
The public comment period closes June 9, 2026, giving hospitals a narrow window to formally shape the final model design.
CJR-X Model Implementation Timeline: Key Dates for Hospital Leaders
- April 2016 – December 2024: Original CJR Model runs in 34 MSAs across approximately 324 hospitals. Strong savings and quality evidence accumulated over 8 performance years.
- January 2026: TEAM launched for five surgical episodes, including joint replacements, at 700-plus hospitals in selected markets.
- April 10, 2026: CJR-X proposed in the FY2027 IPPS rule. Public comment period opens.
- June 9, 2026: Comment deadline. Hospitals should submit formal responses now to influence the final model design.
- Late 2026: FY2027 IPPS final rule expected. CJR PY8 final evaluation results also anticipated.
- October 1, 2027: CJR-X Model launches nationwide. Mandatory participation begins for most IPPS hospitals.
How CMS CJR-X and CMS TEAM Fit Together: CMS’s Push Toward Universal Surgical Episode Accountability?
To understand the full scope of what CMS is doing, CJR-X cannot be read in isolation. It is one half of a two-model strategy that, when combined with TEAM, will bring mandatory episode-based payment to surgical care at essentially every IPPS hospital in the country.
TEAM launched in January 2026 and holds approximately 741 hospitals across 188 Core-Based Statistical Areas accountable for five surgical episode types, including lower extremity joint replacement, coronary artery bypass graft, spinal fusion, hip and femur fracture treatment, and major bowel procedures. The episode window is 30 days post-discharge. TEAM applies to hospitals in selected geographic markets designated by CMS.
CJR-X picks up the rest. Starting October 2027, virtually every IPPS hospital not already in TEAM will be required to manage 90-day joint replacement episodes under CJR-X. The two models do not overlap. TEAM hospitals are excluded from CJR-X, and CJR-X hospitals are outside TEAM’s mandatory markets. Together, they are designed to leave almost no IPPS hospital outside some form of mandatory surgical episode accountability.
There are meaningful structural differences between the two models that hospitals need to understand. TEAM uses a 30-day post-discharge window; CJR-X uses 90 days. TEAM covers five surgical episode types; CJR-X is scoped to joint replacement only. TEAM applies at the hospital level across multiple procedure types simultaneously; CJR-X concentrates accountability on one service line with a longer recovery window. For hospitals in TEAM markets, that 90-day lens on joint replacement is already embedded in their episode. For hospitals entering CJR-X, the extended window creates more opportunity to manage post-acute costs but also more exposure if care coordination infrastructure is not in place.
Read together, TEAM and CJR-X signal something CMS has never done before at this scale. The systematic conversion of high-volume surgical care from fee-for-service payment into mandatory episode accountability. The Innovation Center is no longer piloting this concept in selected markets. It is building the infrastructure to make episode-based payment the default for surgical procedures across the Medicare program.
What CJR-X Means for ACOs and Health Systems
For ACOs operating under the Medicare Shared Savings Program or other risk arrangements, CJR-X adds another layer of accountability that can either reinforce or complicate existing value-based care strategies. Hospitals within ACOs will need to align their CJR-X episode management with broader population health infrastructure, especially around care transitions, post-acute network management, and data sharing with partner providers.
Health systems with multiple hospital campuses face the additional complexity of harmonizing episode performance across sites with different orthopedic volumes, case mixes, and PAC referral patterns. Systems that have already invested in bundle readiness through BPCI Advanced or TEAM will have a meaningful head start. But the nationwide scope of CJR-X means that even hospitals with no prior episode-based payment experience will be brought into the program.
CJR-X arrives at a financially difficult moment for orthopedic programs. Primary total joint arthroplasty reimbursement has declined roughly 56% in real terms since 2000. The 2026 Physician Fee Schedule added another 2.5% efficiency cut on surgical procedures. At the same time, demand for hip and knee replacements is projected to nearly triple by 2040. Layering
mandatory episode accountability on top of compressed procedural payment means hospitals must capture value through care redesign, not through volume alone.
Gainsharing and physician alignment are central to making CJR-X work in practice. Hospitals that cannot distribute shared savings to the surgeons driving episode cost decisions will struggle to change referral behavior, implant selection, and post-acute placement patterns. The expansion of coverage to outpatient settings also raises meaningful questions about how episode accountability applies as LEJR volume continues migrating to ambulatory surgery centers and hospital outpatient departments. Hospitals and ASC partners will need clear agreements on how reconciliation payments and downside risk flow across sites of care.
How Persivia CareSpace® Supports CMS CJR-X Readiness
CJR-X introduces 29 risk adjusters into target price calculations. Hospitals that fail to capture patient complexity accurately will be measured against a target that does not reflect their true case mix. Below are the six operational domains where documentation, coordination, and execution determine whether a hospital earns shared savings or faces repayment, and where Persivia CareSpace® provides the infrastructure to compete.
Persivia has a track record in episodic payment models. CareSpace® has helped health systems improve HCC documentation accuracy and achieve measurable RAF lift under episode-based programs. To see how it worked in practice, download the case study.
- HCC Documentation and Risk Adjustment: Accurate HCC documentation shapes the risk-adjusted target price CMS assigns to each episode. Comorbidities that are present but under documented, such as chronic kidney disease, heart failure, and diabetes with complications, produce a lower target price that does not reflect actual episode cost. CareSpace® flags HCC gaps ahead of the episode, giving CDI teams time to query with specificity before reconciliation puts the hospital at a disadvantage.
- Care Coordination Across the 90-Day Episode: Hospital accountability does not end at discharge. It runs through 90 days of recovery, covering every service the patient touches along the way. CareSpace® tracks each episode longitudinally across inpatient, claims, and post-acute data, giving care coordinators a single view of where each patient stands and surfacing gaps in follow-up before they become costly complications.
- Post-Acute Care Network Management: PAC spending drove most of the savings in the original CJR program, and it remains the largest cost lever under CJR-X. Referral decisions based on historical relationships rather than performance data leave money on the table. CareSpace® supports PAC network tracking at the facility and episode level, giving referral teams the cost, readmission, and outcome data to place patients with partners whose performance holds up.
- Analytics for Target Price vs. Actual Spend: Episode performance is invisible without claims data that spans the full 90-day window across Part A and Part B. CareSpace® gives finance and service line teams a running view of episode spend against target price, broken down by surgeon, DRG, and PAC site, and flags high-cost cases early enough to act rather than simply account for them at year-end.
- Readmission Prevention: An unplanned readmission within the episode window raises actual spend and threatens quality score eligibility for reconciliation payments simultaneously. CareSpace® stratifies LEJR patients by readmission risk, supports structured post-discharge outreach, and shares a line of sight into patient recovery with home health and SNF partners, so warning signs reach coordinators before they reach the ED.
- Quality Measure Performance: Meeting the minimum quality threshold is a prerequisite for receiving any reconciliation payment under CJR-X, regardless of how well a hospital manages episode cost. CareSpace® tracks claims-based quality outcomes, making it possible to identify and address performance variation through peer review and care pathway work before composite scores are locked at the close of a performance year.
Conclusion
The public comment period for CJR-X closes June 9, 2026. Hospitals and health systems have a direct opportunity to shape the final model design, whether on risk adjustment methodology, stop-loss protections, quality measure specifications, or the treatment of safety-net institutions.
Beyond commenting, the time to stand up internal readiness workgroups is now. Bringing together orthopedic surgery leadership, finance, clinical documentation improvement, care management, and population health under a shared CJR-X preparation mandate gives hospitals the best chance of being operationally ready well before the October 2027 launch. Waiting for the final rule before beginning means building in under 12 months what should take 18 or more to do well.
To learn how CareSpace® supports episode-based payment readiness, reach out to the Persivia team directly.
Frequently Asked Questions About the CJR-X Model
- Which hospitals are required to participate in CJR-X?
- Nearly all IPPS-paid hospitals nationwide would be required to participate if CJR-X is finalized. The only exclusions at launch are hospitals already enrolled in the mandatory Transforming Episode Accountability Model (TEAM) and hospitals in Maryland.
- When does the CJR-X Model begin?
- The proposed start date is October 1, 2027. The FY2027 IPPS final rule, expected in late 2026, will confirm the launch date and any modifications to the proposed model.
- What surgeries are covered under CJR-X?
- CJR-X covers lower extremity joint replacement (LEJR) surgeries, including total hip replacements, total knee replacements, and, for the first time, ankle replacements. Coverage applies to both inpatient and outpatient hospital settings.
- How is the CJR-X target price calculated?
- CMS uses a risk-adjusted methodology with 29 patient-level risk adjusters, compared to just 3 in the original CJR program. Accurate HCC documentation is critical because under documented comorbidities produce a lower target price that does not reflect actual episode cost.
Table of Contents